Wife of Ariz. treasurer dies after childbirthFor the rest of the article, go --->hereLike any couple expecting their first child, state Treasurer Dean Martin and his wife were jubilant about the coming addition to their family.
Dean Martin liked to refer to the child as "LT," for "Little Treasurer," and made up a baby outfit bearing the words, "Deposits up front, withdrawals in back."
Martin's joy turned to anguish late Monday, when his wife, Kerry Martin, died of complications from childbirth, a rare event that stunned friends and colleagues. Martin stood vigil at the bedside of his son, Austin Michael Martin, who was listed in critical condition Tuesday at an undisclosed hospital.
Kerry's death saddened city employees in Phoenix, where she worked to promote youth-swimming programs, and shocked those at the state Capitol, where her husband rose quickly from the Legislature to become a statewide elected official poised to one day run for governor.
Kerry, 34, died at 11:53 p.m. Monday, about four hours after delivering an 8-pound, 21.5-inch baby boy. Dean's spokeswoman, Kimberly Yee, would not say what complications led to Kerry's death, or in what hospital the death occurred.
"Words cannot describe the grief I share with so many due to the sudden and tragic loss of Mrs. Kerry Martin," Gov. Jan Brewer said in a statement.
"Kerry was a kind, hard-working, eternally optimistic young lady, a tremendous leader in her own right."
Thursday, May 28, 2009
Wife of Ariz. treasurer dies after childbirth
Friday, May 22, 2009
mother/child connection
 A brief history first...
A brief history first...When Manny was born (pictured left) I had a difficult time connecting with him. I think there were several reasons for this:
1) Becoming pregnant was a HUGE surprise. I was fairly young, 23, and in retrospect I wasn't ready to become a parent. I also feel that I was very removed from the pregnancy. It didn't hit home that I was going to be a Mommy until he was placed in my arms after birth.
2) He was born by cesarean. I didn't go into labor at all. It is well known that being in labor releases "love hormones", also known as oxytocin, which enables a mother to fall in love with her baby. Oxytocin is also released during breastfeeding, and sex. Although a woman's oxytocin level is the highest it will ever be in her life after birth, and this peak is vital.
3) I didn't breastfeed (again, didn't release oxytocin, the love hormone).
4) He was a super fussy, and super needy baby. I often felt resentment toward him. I am sure that I had postpartum depression, but never saw anyone for it, because I felt ashamed of my feelings.
Because of all of the physical and emotional disconnect, I didn't start feeling maternally bonded to Manny until he was close to 4 months of age.
 Christian was a vaginal birth (VBAC). One of the (many) reasons I decided to give birth vaginally was to see if the studies I had read about oxytocin held any water. Obviously I am only one person, so my experience was purely anecdotal, but it was an idea that intrigued me.
Christian was a vaginal birth (VBAC). One of the (many) reasons I decided to give birth vaginally was to see if the studies I had read about oxytocin held any water. Obviously I am only one person, so my experience was purely anecdotal, but it was an idea that intrigued me.Either way, when I finally pushed Christian out we had a connection that can not be denied or described. I immediately knew that he was MY baby, and even though I only saw his face for a matter of seconds before they whisked him away to do the "standard" procedures (height and weight check, as well as APGARs - we declined the vitamin K drops as well as the Hep B shot) I could have picked him out of a line up of newborns.
I was also determined to breastfeed Christian until he was 12 months old. It wasn't easy, and there were definitely moments - especially in the beginning - when I wanted to throw in the towel. But the moment that I brought Christian to my breast all of those feelings disappeared, and I did breastfeed him until 12 months, when he weaned himself.
 John and I have completely opposite relationships with our children. John was always closest to Manny. He was able to tell what Manny wanted before he could speak his mind. He always knew the right way to hold him, the right way to put him to sleep, and he was always the one Manny turned to when he was upset.
John and I have completely opposite relationships with our children. John was always closest to Manny. He was able to tell what Manny wanted before he could speak his mind. He always knew the right way to hold him, the right way to put him to sleep, and he was always the one Manny turned to when he was upset.I was a bit envious of John's relationship with Manny. I assumed that because I was his mother, I would be the one who would instinctually know what to do. However, my instincts failed me. I was a fish out water. I found that the simplest tasks made me frustrated. And I was so happy to have a partner that supported me, and our child.
However, once Christian was born, I knew our relationship would be different. We connected the moment he was born, and the bond grew deeper every day.
The parental roles had suddenly reversed. I was the one who knew what Christian needed, even as a 3 day old newborn. I was the one who knew how to put him to sleep. Since we were mostly breastfeeding (supplementing with formula once a night) he was dependent on me for his meals. And since he wouldn't take a pacifier, he needed me (well, my boob...LOL) to calm his tantrums. Our connection was so deep, that I often woke in the middle of the night right before he did. I suppose my body could sense that he was about to wake up to feed. My milk would even begin to "let down" before he stirred.
Fast forward to the present day.
Over the last month or so I've had insomnia. My sleeplessness isn't consistent. Some days I fall asleep fairly easily, other days I require a bit of help. However it seems that when I have trouble sleeping, Christian does as well.
The first time it happened, I considered it a fluke. It was 2:00 in the morning. I was on the computer. The rest of the house was quiet. All of a sudden I hear Christian shrieking. I let him cry just for a couple of moments (hoping that he would fall back asleep) before I went in to calm him. He quickly fell back to sleep once in my arms.
When it happened the second night I couldn't fall asleep, I considered it a coincidence. When it happened a third time, I wondered if he could sense that I was awake.
Is our mother/child connection so strong that he can sense when I'm awake? It's a bit odd that I just happen to be awake on the nights that he has trouble sleeping. I'm sure that this is a question that can never be fully answered. John and I plan on having at least one more child, which we're hoping will be a homebirth. We'll see if I have the same kind of connection with that child :)
Thursday, May 21, 2009
controlled uterine rupture
 I always read before I go to bed. One (of the many) books I'm currently reading is Pushed by Jennifer Block. The section (no pun intended) I was reading was in reference to the dwindling VBAC rate (now 6.4% a 67% decrease since 1996) and how many, many women are being "pushed" into repeat cesareans, home birth, and even unassisted birth (births where no medical supervision is present).
I always read before I go to bed. One (of the many) books I'm currently reading is Pushed by Jennifer Block. The section (no pun intended) I was reading was in reference to the dwindling VBAC rate (now 6.4% a 67% decrease since 1996) and how many, many women are being "pushed" into repeat cesareans, home birth, and even unassisted birth (births where no medical supervision is present).I started reading this book at 11ish this evening and was finally getting drowsy by midnight. However one of the passages has kept me awake, and I know that I won't be able to sleep until I get this off of my chest.
The following passage is how far (literally, in miles) women will go to have a normal physiological birth:
A woman in Alaska recalled traveling 280 miles from her home of Homer to Anchorage to give birth in a hospital that would allow a VBAC. A woman in Dallas, Texas, recalled firing her midwife the day before she gave birth vaginally, at home, after two prior cesareans. A woman seeking a VBAC in South Dakota traveled to midwives in Nebraska after being refused care by every local doctor, even though she'd already delivered twins vaginally since the cesarean. A woman in Georgia wrangled two out-of-state midwives who drove 5 hours to attend her home VBAC of twins.Reading this deeply saddens me. I am so saddened that women have to go to such lengths to have the birth they desire. Physicians tout the option of "choice" when they speak of elective cesarean, yet they offer no "choice" to women who choose to birth vaginally.
And then there are women on the list who feel they have no other option but to go it alone, to give birth "unassisted," without even a midwife.
What you've got here are people who would rather have a controlled rupture of the uterus - what is a c-section but a controlled rupture of the uterus? -- Linda Bennet, Miwdife (Pushed, by Jennifer Block)
Wednesday, May 20, 2009
L.A. Times Article - Childbirth: Can the U.S. improve?
Once reserved for cases in which the life of the baby or mother was in danger, the cesarean is now routine. The most common operation in the U.S., it is performed in 31% of births, up from 4.5% in 1965.
With that surge has come an explosion in medical bills, an increase in complications -- and a reconsideration of the cesarean as a sometimes unnecessary risk.
It is a big reason childbirth often is held up in healthcare reform debates as an example of how the intensive and expensive U.S. brand of medicine has failed to deliver better results and may, in fact, be doing more harm than good.
...
The problem, experts say, is that the cesarean -- delivery via uterine incision -- exposes a woman to the risk of infection, blood clots and other serious problems. Cesareans also have been shown to increase premature births and the need for intensive care for newborns. Even without such complications, cesareans result in longer hospital stays.
Inducing childbirth -- bringing on or hastening labor with the drug oxytocin -- also is on the rise and is another source of growing concern. Experts say miscalculations often result in the delivery of infants who are too young to breathe on their own. Induction, studies show, also raises the risk of complications that lead to cesareans.

To read the rest of the article go --->here.
The article goes on to say that despite all of these medical interventions, which the public is led to believe are needed in order to "save lives" (and in some cases are needed and do save lives, I won't deny that), the U.S. maternal morbidity rate continues to rise.
According to recent figures, the U.S. maternal mortality rate was 13 deaths per 100,000 live births in 2004. The rate was 12 deaths per 100,000 live births in 2003 -- the first year the maternal death rate was more than 10 since 1977 (Stobbe, AP/Washington Post, 8/24). A total of 540 women were reported to have died of maternal causes in 2004, 45 more than were reported in 2003, according to the report (NCHS report, 8/21).(1)
What is causing the morbidity rate to rise? Some speculate that obesity, maternal age as well as ethnicity are all factors. However, according to a review of maternal deaths in New York, excessive bleeding is one of the primary causes of pregnancy-related death, and women who have undergone several previous c-sections are at particularly high risk of death.(2)
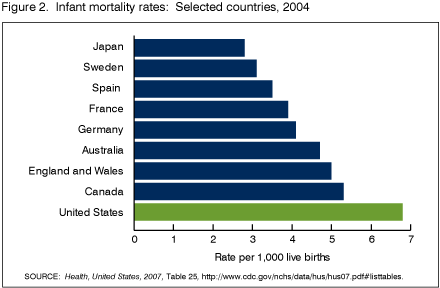
In conjunction, the U.S. has the highest infant mortality rate amongst developed countries (ranking 29th in the world). The CDC reports that in 2006 the infant mortality rate was 6.71 deaths per 1,000 births.
What is the leading cause of infant death? Prematurity. In 2005, 68.6% of all infant deaths occurred to preterm infants, up from 65.6% in 2000.(3)
 Unfortunately the reason for preterm birth is unknown. However, with the recent rise of "late preterm birth" (infants born at 34–36 weeks gestation) one could guess that the rise in cesarean births could play a part. However, in order to be fair, we must also take into account the rise in multiple births as well as socioeconomic status.
Unfortunately the reason for preterm birth is unknown. However, with the recent rise of "late preterm birth" (infants born at 34–36 weeks gestation) one could guess that the rise in cesarean births could play a part. However, in order to be fair, we must also take into account the rise in multiple births as well as socioeconomic status.I will end this blog with the thoughts of Kristie McNealy, MD:
The question is why? If we can keep a 22 weeker alive, why can’t we keep babies inside their mothers, growing and healthy?Good question Kristie, good question.
For the rest of the CDC report on infant mortality go ----> here.
To read the rest of Dr. McNealy's article go ---> here.
Monday, May 18, 2009
the sphincter law
 After many recommendations I recently started reading Ina May Gaskin's (picture left) book, Ina May's Guide to Childbirth. It truly is a fascinating book.
After many recommendations I recently started reading Ina May Gaskin's (picture left) book, Ina May's Guide to Childbirth. It truly is a fascinating book.For those of you who are not familiar with Ina May, I'll give a brief background....Ina May Gaskin is a midwife who, in 1971, along with her husband Stephen, founded The Farm in Lewis County, Tennessee (near the town of Summertown). Each year hundreds of women flock to The Farm to give birth.
Ina May Gaskin is one of the Founders and the current president of the Midwives' Alliance of North America. She is a powerful advocate for a woman's right to give birth without excessive and unnecessary medical intervention.
Her clinical midwifery skills have been developed entirely through independent study and apprenticeship with other midwives around the world. Ina May and fellow Farm midwives were instrumental in the development of the rigorous Certified Professional Midwife (CPM) certification process (1).
Ina May has authored two books. The first book she wrote was entitled Spiritual Midwifery, which I have not yet read. Her second book is Ina May's Guide to Childbirth (IMGC).The first half of IMGC consists of birth stories. However, these aren't your typical birth stories. In this day and age when a pregnant women hears birth stories from her relatives or friends, they almost always start with an induction (either with cervidil or artificial rupture of membranes), followed by pitocin and eventually an epidural. Rarely do women hear stories of natural childbirth. If they do, it's most likely a horror story about a woman who was "forced" into an unmedicated birth (i.e. a woman who progressed too quickly and wasn't able to get an epidural) and hated every minute of it.
However in IMGC birth is something to be celebrated. These women go into labor believing that birth is a natural process. They aren't afraid of it, they embrace it. I have never encountered a book where every story I read was a story of a natural, unmedicated, healthy labor. When I become pregnant for the final time, I will saturate my soul with these kinds of stories.
One of the "laws" that Ina May discusses in IMGC is The Sphincter Law.
Let me play out a scenario that I'm sure some of you are familiar with...it's mid morning, and you have just enjoyed your first (perhaps only) cup of coffee. Shortly after your bowels start hinting that it's time to visit the restroom. You eventually make your way to the bathroom and find yourself constipated. You tighten your jaw, clench your teeth, and beg for relief. Nothing happens. Perhaps you're like my husband and the only place that you can relieve yourself is in your own bathroom at home (I'm sure he'll love that I've shared that bit of information with you...LOL). And why is that? Because home is comfortable, you can relax and let nature take it's course.
The uterus, like the anus, is a sphincter muscle. It does not obey on command. It works best when the laboring mother is comfortable, and surrounded by familiarity. It can also "slam shut" if the laboring mother becomes frightened.
How does one relax the sphincter of the uterus? One of the suggestions that Ina May gives is laughter. Laughing opens and relaxes your mouth. Relaxation of the mouth directly correlates with the ability of the cervix, the vagina and the anus to open to full capacity. Other ways include: slow, deep breathing, and warm water. But most importantly a Ina May suggests that trust and love make relaxation possible. Because Trust is such a valuable and powerful feeling, it is important for pregnant women to be cared for by people whom they trust. (2)
"Sphincters may "slam shut" without the volitional act of their owner. The sudden contraction of previously relaxes sphincter muscles is a fear-based reaction. This is part of the natural fight-or-flight response to perceived danger. Adrenaline/catecholamines rise in the bloodstream when the organism is frightened or angered. Female animals in labor in the wild, such as gazelles and wildebeest, can be on the point of giving birth and yet can reverse the process if surprised by a predator." -- Ina May Gaskin, Ina May's Guide to Childbirth
Below is a video of Ina May discussing the power of the Sphincter Law at The Farm in Tennessee...
Midwife Ina May Gaskin Talks About Natural Childbirth - 2 -
Let's recap:
- Sphincter muscles of both anus and vagina do not respond on command.
- Sphincter muscles open more easily in a comfortable intimate atmosphere where a woman feels safe.
- The muscles are more likely to open if the woman feels positive about herself; where she feels inspired and enjoys the birth process.
- Sphincter muscles may suddenly close even if they have already dilated, if the woman feels threatened in any way.
2, Ina May Gaskin's Guide to Childbirth, Ina May Gaskin
Friday, May 15, 2009
the benefits of vernix
I will say though that Manny was immediately washed after he was born. He has grown into completely healthy 3 year old. He suffered no major illnesses as an infant. Christian wasn't bathed immediately, but he was bathed within the first 24 hours, and he is a completely healthy 13 month old. However I do think it's important to know that there are benefits to delaying a newborns first bath. After reading the information, you make the decision that is best for you.
 When a baby is born he is covered in a waxy white substance (some say it also looks like cheese). This substance is called vernix caseosa.
When a baby is born he is covered in a waxy white substance (some say it also looks like cheese). This substance is called vernix caseosa. Vernix is secereted by babies sebaceous glands while in utero. It is thought to protect the baby's skin from amniotic fluid. Without this protection baby's skin would become wrinkly (think about how your skin looks after you get out of a pool or bath). It is also thought that vernix has antibacterial properties to protect baby from infections while inside the uterus.
At the time of birth one of the standard procedures followed by hospitals is to immediately bathe a newborn. Unfortunately - it is believed by some - that this procedure does more harm than good. Several studies have shown that leaving vernix on a newborn for several days (some suggest until a good breastfeeding routine has been established) could protect him from bacteria in his new surroundings.
"Antimicrobial Properties of Amniotic Fluid and Vernix Caseosa Are Similar to Those Found in BreastmilkAnother study:
Akinbi, H. T., Narendran, V., Pass, A. K., Markart, P., & Hoath, S. B. (2004). Host defense proteins in vernix caseosa and amniotic fluid. American Journal of Obstetrics and Gynecology, 191 (6), 2090-2096. [Abstract]
Summary: In this study, researchers analyzed samples of amniotic fluid and vernix caseosa (vernix) from healthy, term gestations to determine the immune properties of these substances. Participants were pregnant women admitted for elective cesarean section after 37 weeks gestation with no prior labor and no signs of chorioamnionitis (intrauterine infection). Women with a history of prenatal fever or premature rupture of membranes, or who received steroids prenatally or antibiotics during delivery were excluded, as were women whose babies passed meconium in utero, had congenital malformations, or required prolonged resuscitation after birth. Amniotic fluid was obtained by amniocentesis to determine fetal lung maturity prior to elective delivery. Vernix was gently scraped from the newborn's skin with a sterile implement immediately following delivery. There were 10 samples of amniotic fluid and 25 samples of vernix obtained.
Tests (Western analysis and immunochemistry) revealed that lysozyme, lactoferrin, human neutrophil peptides 1-3 and secretory leukocyte protease inhibitor were present in the amniotic fluid samples and in organized granules embedded in the vernix samples. These immune substances were tested using antimicrobial growth inhibition assays and found to be effective in inhibiting the growth of common perinatal pathogens, including group B Streptococcus, K pneumoniae, L monocytogenes, C albicans, and E coli.
The authors point out that the innate immune proteins found in vernix and amniotic fluid are similar to those found in breast milk. As the baby prepares for extrauterine life, pulmonary surfactant (a substance produced by the maturing fetal lungs) increases in the amniotic fluid, resulting in the detachment of vernix from the skin. The vernix mixes with the amniotic fluid and is swallowed by the growing fetus. Given the antimicrobial properties of this mixture, the authors conclude that there is therefore "considerable functional and structural synergism between the prenatal biology of vernix caseosa and the postnatal biology of breast milk." They also suggest that better understanding of these innate host defenses may prove useful in preventing and treating intrauterine infection.
Significance for Normal Birth: It is well understood that routine artificial rupture of membranes increases the likelihood of intrauterine infection because it eliminates the physical barrier (the amniotic sac) between the baby and the mother's vaginal flora. This study suggests an additional mechanism for the prevention of infection when the membranes remain intact: a baby that is bathed in amniotic fluid benefits from antimicrobial proteins that are found in the fluid and in vernix caseosa.
The results of this study also call into question the routine use of some newborn procedures. Early bathing of the baby removes vernix, which contains antimicrobial proteins that are active against group B streptococcus and E. coli. Delaying the bath and keeping the newborn together with his or her mother until breastfeeding is established may prevent some cases of devastating infections caused by these bacteria. The fact that preterm babies tend to have more vernix than babies born at or after 40 weeks might mean that healthy, stable preterm babies derive even greater benefit from staying with their mothers during the immediate newborn period.
Finally, this study illustrates how the normal physiology of pregnancy and fetal development is part of a continuum that extends beyond birth to the newborn period. The immunologic similarities between amniotic fluid, vernix and breast milk provide further evidence that successful initiation of breastfeeding is a critical part of the process of normal birth."
Is vernix caseosa a protective material to the newborn? A biochemical approach.
Baker SM, Balo NN, Abdel Aziz FT.
Department of Nursing, Al-Arab Medical University, Faculty of Medicine, Benghazi, Libya.
Twenty random samples of vernix caseosa were collected from immediately born neonates, in Jamahiriya Hospital, Benghazi. Biochemical studies of these samples revealed presence of lipids (62.5%), proteins (36%) and carbohydrate (1.5%). Also we could observe inhibition of staph. aureus and klebsiella growth on nutrient agar by this vernix. This observation could be explained either by its higher asparagine content or by its elevated lipid component. In addition tripalmitin was found to be the major lipid constituent, responsible for its hydrophobic property. So we recommend leaving this vernix layer on newborn skin until spontaneous drying.A novel role for vernix caseosa as a skin cleanser.
Moraille R, Pickens WL, Visscher MO, Hoath SB.
Division of Neonatology and Skin Sciences Institute, Cincinnati Children's Hospital Medical Center, Cincinnati, Ohio 45229, USA.
OBJECTIVES: Skin cleansing is a complex process involving endogenous and exogenous mechanisms. This study examines the role of vernix caseosa in the process of skin cleansing in the perinatal period.METHODS: Vernix was evaluated as an exogenously applied skin cleanser using digitized image analysis which quantified residual carbon particles following a standardized cleansing assay. In addition, the detachment of vernix from human cadaveric skin and Gore-Tex supports was investigated following timed exposures to a variety of commonly used commercial surfactants. Detachment was quantified spectrophotometrically as increased turbidity at 650 nm.
RESULTS: Image analysis showed that exogenous application of vernix exhibited a cleansing capability comparable or superior to standard skin cleansers. Dose-dependent increases in solution turbidity (vernix detachment) were seen following exposure of vernix-covered Gore-Tex vehicles to sodium laureth sulfate, sodium lauryl sulfate, and cocamidopropyl betaine solutions. Similar results were seen with cadaveric skin.
CONCLUSIONS: These results demonstrate a role for vernix caseosa as a skin cleanser. Previous views of vernix as a soil or skin contaminant at birth need to be reevaluated.
Thursday, May 14, 2009
tokophobia
 After writing my first blog yesterday (found here), I started thinking about fear in childbirth; not too long ago I was educated about an anxiety disorder called tokophobia.
After writing my first blog yesterday (found here), I started thinking about fear in childbirth; not too long ago I was educated about an anxiety disorder called tokophobia.Tokophobia is a a fear of childbirth (from the Greek tokos, meaning childbirth and phobos meaning fear). This fear stems so deeply that women who suffer this traumatic disorder usually don't bare children, though many of them desire babies of their own. If they do become pregnant, they typically request cesarean sections.
Dame Helen Miran spoke of her fear of childbirth in a British magazine in October of 2007. As a young girl - 13 years of age - in Catholic school she was shone a traumatizing video of a birthing mother (sound familiar?). This video jaded her perception of childbirth. As such, she never became a mother.
You can read the rest of her story here.
There are many variables which can cause this anxiety disorder. If a mother has a traumatic birth experience and shares that experience to the fullest detail with her daughter (i.e., "labor is the worst pain I've experienced in my life!", "I had a 4th degree tear that ripped through to my anus!"), her daughter could possibly garner a fear of childbirth. Women who've experienced sexual abuse as a child may have fear of vaginal exams. If a woman has had a family member die in labor, that could cause her fear; as well as previous traumatic birth experiences by the mother herself.
Below are some articles that discuss tokophobia to great lengths. The first article I found the most interesting. It consists of a study that took place in United Kingdom at Queen Elizabeth Psychiatric Hospital in Birmingham. Twenty six women were included in the study, the findings are very interesting.
Of the 26 patients, 8 of the patients had primary tokophobia, that is their fear of childbirth predated their pregnancies. Of these 8 women 4 achieved their perfect birth, and had no problem bonding with their children. The remaining women had vaginal births (most against their will), where two suffered PTSD.
The remaining 14 women in the study had secondary tokophobia, their fear developed after the trauma suffered from their first births. One woman of the 14 had an abortion (rather then face another delivery) when she became pregnant with her second child. Several had miscarriages, and one had an ectopic pregnancy. These women were pleased that their pregnancies had to be terminated.
You can find the rest of the study here.
Here is another article: Tokophobia: Fear of Pregnancy and Childbirth
Do I think I suffered from tokophobia. Perhaps. The thought of labor frightened me so much that I longed for a c-section. However I was never so afraid that I wanted to terminate the pregnancy.
Unfortunately tokophobia isn't a widely known disorder. Fear and anxiety are common emotions for first time mothers, and I have a feeling that those who express these concerns are told that what they are feeling is normal.
I also believe that the enormity of the disorder is not well known. I would imagine feeling complete dread over childbirth can cause embarrassment. As such, I'm sure some women keep their feelings to themselves, never telling a soul of the anxiety that they feel whenever they see pictures of birthing mothers, or hearing birth stories.
This is why I try not to pass judgment of others birth choices. You never know their back story. Perhaps the woman that you were speaking to today about her scheduled cesarean is tokophobic. Would you begrudge her her ideal birth just because you do not agree with her choice?
Wednesday, May 13, 2009
her-story (part 3)
 My Journey to VBAC
My Journey to VBACWhen I found out I was pregnant with baby #2 I hadn't even considered VBAC. I was under the impression that "once a c-section always a c-section" applied. Luckily I belonged to a message board where, only months earlier, a poster went on her own VBAC journey. Her story inspired me. She wasn't afraid of labor, she embraced it. She was strong. She was empowered, and I wanted to experience that too.
I still toyed with the idea of a repeat c-section. There were a couple of minor benefits: 1) I knew what to expect, and 2) I could schedule the delivery, making it easier to arrange childcare. However, I knew that if I were to have a 2nd c-section that would be it. I would always have my children delivered for me. Was that something I really wanted? Would I regret not even trying to birth?
I started to do some research. I wanted to see what child birth could be like. I looked up birthing videos on youtube. I started to read birth stories. Yes there is pain involved with labor, but once a mother pushes her baby out the pain disappears and a feeling of euphoria emerges. I wanted to experience that. I never had that euphoric feeling with Manny. Did I love my son? Of course. Was I happy to become a mother? Of course, but seeing how happy these women were made me jealous. I wanted to experience what they had experienced. In my 4th month I finally decided that I would birth my baby the way nature had intended.
The last 5 months of my pregnancy consisted of becoming as well versed in the subject of VBAC as humanly possible. I studied rupture rates (less then 1%). I learned what to avoid in order to make my birth a success (prostaglandin induction, artificial rupture of membranes (AROM), pitocin, epidural, purple/directed pushing in the lithotomy position). Unfortunately I couldn't afford any childbirth prep courses, so I bought as many books, on as many subjects as I could. I felt that I was prepared for any and everything.
I had learned that having a doula would increase my chances of success, but unfortunately that wasn't something we could afford either, so I tried to have John read as much as possible. We would do fine...or so I thought.
Unfortunately I was racing the clock. My doctor didn't feel comfortable with me going past 40 weeks. I told her that I wasn't comfortable scheduling my c-section before 42 weeks. We made a compromise, and I would be having a repeat c-section if I didn't go into labor, on my own, before 41 weeks 1 day.
At 40 weeks 2 days I went into early labor. Contractions started that evening. It was Friday night and I was contracting every 10-15 minutes. The contractions continued through the night. They were uncomfortable, but not unmanageable. I slept (restlessly) about 4 hours that evening. By Saturday morning I was contracting every 5 minutes. Again the contractions were uncomfortable, but not unbearable. We called my dad that morning around 8:00 a.m. and told him that he would need to make his way over to our house.
John and I left for the hospital at 12:00 p.m. I was admitted to triage where they hooked me up to a bunch of monitors, and checked my dilation...I was ONLY 2 friggin' centimeters! My worst fear had been realized. I had been up ALL night with contractions, and they weren't doing a damned thing!
Here is where the cards started stacking against me: because I was a VBAC patient I was admitted into the hospital. If I were a regular laboring mother, I most definitely would have been sent home. I was immediately wheeled into a birthing suite, where again, I was monitored for 20 minutes.
Over the course of the following (several) hours I walked, I showered, I bounced on a ball. Contractions were about 3-5 minutes apart, and becoming increasingly painful, so much so that I had to stop everything I was doing to make it through them. John helped me as best he could, but he could definitely see that I was starting to crumble. If I stayed on top of the contractions I was able to handle them, but the moment that I "let loose" I fell apart.
 After what seemed like an eternity the nurse came and checked me again. I was still only 2 centimeters! I just about died. I was losing my resolve. I let the fear seep in. If these contractions were this painful, how in the HELL could I handle active labor, or even transition!?! I lasted another hour before I begged for the epidural.
After what seemed like an eternity the nurse came and checked me again. I was still only 2 centimeters! I just about died. I was losing my resolve. I let the fear seep in. If these contractions were this painful, how in the HELL could I handle active labor, or even transition!?! I lasted another hour before I begged for the epidural.I knew what would happen after I got the epidural. I had read about it in EVERY book that I bought. I was warned about the procedures that would follow, and was told to avoid them at all costs. Unfortunately that epidural sealed my fate.
Two hours after getting the epidural my bag of waters was artificially ruptured. Several hours after that I was given a low dose of pitocin. I told the nurse that I didn't want the pitocin, but she told me that my contractions weren't strong enough, or consistent. I was assured that they'd keep a close eye on the strength and length of the contractions, and if they thought for even a half of a second that something was wrong, they would shut it off. I conceded and the pitocin drip started. Every couple of hours the nurse would come in, and turn the pit drip up. This continued until they were sure that I was in transition. The last number I remember on the pit machine was 12.
I spent the rest of the day in and out of sleep. I was starving, but was refused food. John went down to get some lunch. I had him sneak me some snacks.
Oddly enough I could feel myself hit transition. One moment I was feeling fine. The next I could feel intense pressure in my abdomen, as well as some cramping. Shortly after, I barfed up the croissants that John had brought me.
I was complete at 11:00 p.m. on Saturday, March 22nd. I realized how close I was to midnight and asked if we could wait. My Grandma's birthday is March 23rd, and I thought it would be awesome to have Christian born on her birthday. I was told that I was at -1 station, so we needed to wait a bit anyway. The nurse tilted my bed to a 40 degree angle so that gravity could take over.
I started pushing at 12:15 a.m. I couldn't feel any contractions, so I had to have directed pushing in the dreaded lithotomy position (flat on my back). On counts of ten I held my breath and "bared" down.
 Christian was born at 12:45 a.m. March 23rd (Easter Sunday) and I had given birth to him vaginally. I suffered a 2nd degree tear to my perineum, as well as several small tears to my labia.
Christian was born at 12:45 a.m. March 23rd (Easter Sunday) and I had given birth to him vaginally. I suffered a 2nd degree tear to my perineum, as well as several small tears to my labia.For several days (possibly weeks) following Christian's birth I was on a high. I was so proud of myself for birthing my baby. It wasn't until I had a moment to catch my breath that I realized Christian's birth didn't go at all how I had planned.
I know exactly where I went wrong: 1) I went into the hospital too early, 2) I got an epidural too early. Had I waited on both of the aforementioned, I know that I wouldn't have had all of the interventions that I did have.
I know exactly what I would do were I in that situation today:
- hired a doula, this is a biggie. I know hiring a doula would have changed the entire tone of my labor. I think I expected too much from John. I think we, as woman, have a tendency to do that to our husbands/significant others. Childbirth isn't their "realm", and it was unfair for me to put that kind of pressure on his shoulders.
- stayed at home longer.
- not gotten an epidural, or wait at least until I was in active labor to get one. I would also request to have the epidural turned off during the pushing phase.
her-story (part 2)
 Ignorance is Bliss
Ignorance is BlissAt the age of 23 I found myself in a loving, stable relationship of 4 years. I also found myself unexpectedly pregnant. Oddly enough, the moment I found out I was pregnant (at such a young age) I wasn't scared of my emotional well-being (that came later) I was scared of birthing my baby.
The 9 months following my positive home pregnancy test were fairly easy. I had horrible morning sickness for the first four months (I figured this was my penance for being irresponsible and getting pregnant so young). I was scared to become a mommy at such a young age, but I knew that with the help of my awesome (now) husband, everything would work itself out. But mostly, I was terrified of giving birth.
When a woman finds herself pregnant birth stories come out of the wood work. Horror stories. People feel inclined to tell you how painful child birth is, how much you'll NEED the epidural. They tell you painful stories about episiotomies, and 4th degree tears. Nobody ever tells you that it can be beautiful (I take that back, my mom told it could be beautiful, but I think I tuned her out...haha).
As each month of my pregnancy passed, I prayed that I would need a c-section. For me, it seemed like the ideal option: 1) I wouldn't need to experience labor 2) I wouldn't need to push a baby out of my hoo-ha, and 3) I could schedule when my baby was to be born...PERFECT! Unfortunately, that opportunity never presented itself....until my 38th week well check.
At 38 weeks I found out that my little bun had flipped to breach. I tried not to smile as my doctor told me, but I could feel myself get lighter. I could breath. I could sit up straight. There was nothing to fear. It was as if someone had answered my prayers. I would be getting my c-section!
 On the morning of March 2nd my husband drove me to Mills-Peninsula Hospital at 5:30 a.m. I was prepped and walked myself into the O.R. at 7:30 a.m. Up until that point I wasn't aware of the gravity of the situation.
On the morning of March 2nd my husband drove me to Mills-Peninsula Hospital at 5:30 a.m. I was prepped and walked myself into the O.R. at 7:30 a.m. Up until that point I wasn't aware of the gravity of the situation.I was having surgery today.
I know it's ignorant, but the fact that they would be cutting me open never really bothered me until I was sitting on the operating table. I looked around the room to find a comforting face. The only thing I saw were nurses buzzing around the room preparing for my operation; they're faces covered with masks.
I sat on the cold steel operating table, my gown opened in the back (I was freezing). The anesthesiologist approached me and told me that he would be inserting my epidural. I felt him clean my back, and stick me with a small needle. He told me to expect a lot of pressure as he inserted the catheter.
The epidural took effect almost instantly. I was laid down before my legs went completely numb. As I was laying on the cold table, the weight of my belly made it difficult to breath. My breathing became more labored as the epidural started to work. I felt suffocated, which caused me to hyperventilate. I remember telling the nurse, "I can't breathe!" They tried to comfort me and tell me this was normal. I was told to take long deep breaths. Moments later I started to throw up. Internally I was screaming for my husband. The nurse even asked if she could let him in, but the anesthesiologist didn't think it would be wise to bring him in when I was so distraught.
The rest of the morning is a drug induced blur. Here is what I remember:
- John eventually being let into the O.R.
- Being grossed out at the blood spatter on the drape in front of me.
- Tugging and pulling.
- Manny being pulled out of my belly.
- Being wheeled into the recovery room.
- Waiting (for what seemed like hours) for the anesthesia to wear off.
- Trying to nurse Manny.
When I was discharged I never had my vicodin prescription filled - I didn't need to. I was walking and climbing stairs on day 2 of being discharged. My incision did open slightly, but after seeing a doctor I was told that it had healed enough to where it wasn't a problem.
After some reflection I've decided that my cesarean experience wasn't completely awful. Yes, I was terrified in the O.R. and had a minor anxiety attack. Yes, it is difficult to recall some details of that day because of all of the medication that was flooding my system. But, it could have been a lot worse.
her-story (part 1)
When I was a Sophomore in high school I attended my 4th period Human Development class on a sunny Spring day. This week we were discussing human sexuality. On that particular day we would be discussing child birth. If I'm completely honest I don't remember the lecture at all, what I do remember was the video that was shone.
It was a video of a laboring mother. She was screaming, grunting and breathing rhythmically. She was in transition on the verge of pushing. It was the scariest thing I'd ever seen in my short 15 years on this earth. Moments later the camera moved in between her legs where you could see a bulging perineum. The lips of the womans vagina stretched as a small head made it's way through the opening.
My eyes wide, my chin hitting the top of my desk. I watched in horror as a small human emerged from between her knees. I remember the statement I made at that point, " I will NEVER be doing that!" That evening I told my parents that I would never be birthing my own children. If I felt I wanted to be a mother, I would most certainly adopt.